


Athletes depend on their excellent, strength, flexibility and mobility to be able to perform effectively in their specific sport or physical activity. They undergo rigorous training in order to prepare for competitive seasons. While many athletes understand and use preventive measures to avoid experiencing an injury or developing a condition, the constant utilization of the different structures of the body can gradually cause the degeneration of the tissues, eventually resulting in an unexpected injury. Many athletes commonly experience sports injuries, however, one type of injury can cause tremendous hardships for the affected athlete: a torn meniscus.
Within an incidence ratio of 60 to 70 for each 100,000 visits, meniscal tears of the knee are a common diagnosis among many sports injury scenarios. Meniscal tears have accumulated great amounts of lost time from physical activity and even employment, which is why understanding the risk factors for meniscal tears is essential, allowing for a quicker and more accurate diagnosis of this type of sports injury.
Lesions to the meniscus frequently occur in sport settings where tremendous dynamic demands are placed against the knee during specific movements. Moreover, meniscal tears may also occur during workplace environments where repetitive, constant motions can develop complications.
Basic activities, such as standing, lifting, squatting, kneeling and sitting, are believed to increase the chances of damage to the meniscus. The time between ACL, or anterior cruciate ligament, ruptures and surgical reconstruction procedures have also been acknowledged as a risk factor for meniscal lesions. Numerous elements contributing to this type of injury have been recognized, however, there’s limited research to support them.
Scientists at the University of Amsterdam, published a systematic review along with a meta-analysis, which investigated several key risk factors for meniscal tears.
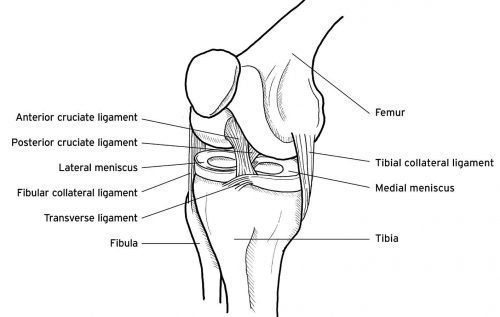
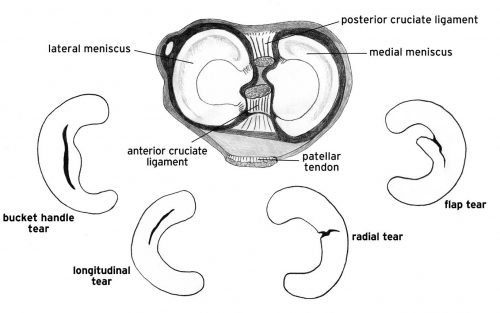
The menisci are two semilunar ridge-like structures, which are positioned on the medial and lateral surface of the tibial plateau. The menisci function by allowing the convex surface of the femur to articulate on the concave surface of the tibia. Additionally, the menisci enable the conversion of weight as well as the absorption of shock during dynamic movements, acting to protect the articular cartilage. Meniscal lesions can be characterized as acute or degenerative, manifesting in different forms, such as a bucket handle tear, a horizontal tear, or a degenerative tear.
Table of Contents
Anterior View Of The Right Knee
Superior View Of Tibial Plateau & Forms Of Meniscal Lesion
Degenerative Risk Factors For A Torn Meniscus
Two research studies concluded that an individual’s body mass index, or BMI, may be consequential with degenerative meniscal alterations. Scientists from Boston University analyzed the BMI of 991 participants, of which 565 were female and 426 were male. The evaluation demonstrated that females with a meniscal tear had a considerably higher BMI, approximately 29.9 percent, than females without meniscal damage, approximately 27.9 percent. Nonetheless, there were no statistical differenced in body mass index for males, with or without meniscal damage. An identical research study distinguished a considerable difference in meniscal tears among participants with a BMI of 25 to 30 kg/m2, a 76 percent of incidence, when compared to participants with a BMI of less than 25 kg/m2, with a 34 percent of incidence. It was concluded, through statistical analysis, that a BMI greater than 25 kg/m2 produced a greater disposition for meniscal damage than those with a lower BMI. It’s essential to keep in mind that these statistics don’t simply involve individuals of obese proportions but it also includes those who maintain a greater muscle mass as well as increased body mass.
As previously recognized in other studies, age is considered to be a critical element for these particular knee injuries. Researchers have confirmed that older individuals may in fact experience greater meniscal trauma. For instance, approximately 19 percent of females and 32 percent of males ranging from 50 to 59 years of age, faced meniscal destruction, in comparison to 51 percent of females and 56 percent of males ranging from 70 to 90 years of age, who presented meniscal trauma. The researchers concluded that people aged 60 years old and over were considerably more probable to suffer from degenerative meniscal tears than someone under 60 years of age. Regardless, the results of the study failed to explain that individual’s younger than the age group provided for the study could also sustain meniscal tears. As a matter of fact, knee complications can also be considered to be some of the most prevalent types of youth injuries, although further research is required to properly determine the statistics of youth athletes with meniscal lesions.
Furthermore, gender has also been considered to be an important risk factor for injuries to the meniscus, as identified in other studies. Additional research from the Boston University evaluated the relationship between meniscal tears, pain and osteoarthritis in 154 patients with identified symptoms of knee osteoarthritis. Using MRI scans, the end results demonstrated that 91 percent of individuals presented a medial or lateral meniscal tear, in which males were identified with a significantly higher prevalence of meniscal lesions than females. Another study distinguished the features of meniscal lesions in 991 individuals through the utilization of MRI scans. Again, males demonstrated a considerably higher incidence of meniscal tears among all age groups, although females diagnosed with meniscal degeneration were categorized within the 70 to 90 years of age group. Whether the higher occurrence of injury in males was due to greater participation in sport or due to occupational activities was not determined in the study.
Three distinct research studies found that kneeling and squatting for more than one hour per day could influence the development of meniscal tears. Individuals whom participate in certain trades or professions, such as carpentry, electrician and plumbing, positions which have widely been occupied by males, repetitively and constantly kneel and squat as a part of their average work day. Research carried out at Southampton University in England determined that 59 participants experienced locking of the knees where 29 were exposed to kneeling and 30 were exposed to squatting in their workplace. Of these 59 individuals, some which may have crossed over in both categories, 69 percent and 73 percent correspondingly consulted an orthopedic surgeon. These participants reported engaging in frequent kneeling and squatting positions while at work, however, several participants also reported participating in specific sports, such as football, which is also considered another risk factor for meniscus lesions.
Sitting for more than two hours per day was believed to decrease the risk of meniscal tears. Two studies conducted by the same leading author from Southampton University, focused to determine the risks of sitting. Also, sitting for extended periods of time was believed to incline an individual to develop other knee conditions, such as patellofemoral pain, also referred to as movie/theatre sign, of which sitting is believed to be a risk factor. Although studies concluded that sitting doesn’t increase the chance of further damaging meniscal tears, it was determined to potentially create issues on other areas of the knee.
Standing or walking for more than two hours per day for 12 months before experiencing symptoms, as compared to less than two hours per day, were thought-out to influence the development of meniscal lesions. Two additional research studies evaluated the effects of standing and walking for extended periods of time. The results concluded that from 71 participants who were disclosed to prolonged standing or walking for more than two hours per day, 54 percent had consulted an orthopedic surgeon due to symptoms of meniscal damage. In comparison, walking and standing was concluded to be effective, in terms of energy expenditure, mechanical bone loading, cardiovascular fitness and overall health, apart from other perspectives.
Walking more than two miles per day within 12 months before symptoms, was determined to have a very low chance of causing meniscal lesions. The health benefits of walking outweigh the possibility of knee injuries and therefore, should not be excluded otherwise unless the symptoms prevent the individual from participating.
Moreover, climbing more than 30 flights of stairs per day within the 12 months prior to the onset of pain and discomfort, was found to considerably affect the individual, aside from climbing stairs 30 times per day, lead to an increased possibility of knee injuries. During a study, 17 male participants reported meniscal related symptoms, such as locking, when climbing stairs, with 59 percent resulting in a consultation with an orthopedic surgeon.
Carrying an excess of 10 kg, 25 kg and 50kg more than 10 times per week concluded in two studies that there was a significant effect against the structures of the knees, increasing the risk of a meniscal lesion.
Acute and degenerative meniscal tears were investigated in a current research study. Utilizing a community sample of 2,806 males in the south of England, by means of a questionnaire, 1,404 participants responded where 762 reported experiencing prior symptoms of knee injury. Of the 762 participants with symptomatic knees, 127 reported symptoms of locking during one or more occupational activities, which lasted longer than 24 hours. The results confirmed a potential increased risk of meniscal lesions within the 20-59 age category.
Acute Risk Factors For A Torn Meniscus
In one study, weight bearing after an individual experienced trauma, concluded to pose a moderate danger for the occurrence of meniscal tears. Researchers from Lund University in Sweden determined that individuals with an ACL injury who engaged in non-weight bearing activities were less likely to sustain further damage to the meniscus. Frequently, ACL injuries occur in load bearing positions which often result in greater joint compression forces of the tibiofemoral compartment. Thus, the well-known term, the unhappy triad, has been more appropriately termed the unhappy compression injury. The unhappy triad refers to trauma involving the ACL, medial collateral ligament and the medial meniscus. It’s ultimately important to stabilize the joint of the knee through the use of conservative or surgical procedures to prevent additional compression against the meniscus. It was therefore concluded that weight bearing during an injury disclosed a moderate chance of injury to the meniscus, however, the authors were unable to determine whether a considerable effect existed.
The participation in any sport or physical activity in general is considered to be a comparably high risk factor for meniscal tears. Two research studies assessed the prevalence of knee injuries during football, rugby, swimming and running. Both football and rugby were concluded to be considerably high components in the incidence of meniscal tears. In comparison, swimming and similar sports were considered to pose a moderate chance of causing meniscal tears. Furthermore, a lack of evidence was unable to determine if running could develop knee complications. Due to the demands of the transfer of mass and the rotational forces applied, it’s not difficult to note how football and rugby could be a potential danger for further injury in athletes with previous meniscus trauma.
Laxity Of The Knee Joint
Anterior cruciate ligament, or ACL, injuries where there’s an extended period of time till an athlete will receive reconstructive surgery have been well recorded as an influence towards the development of meniscal lesions. An ACL deficient knee requires the menisci to function accordingly as a stabilizing component along the posterior-anterior, valgus-varus and internal/external rotation movements. While rehabilitation methods such as chiropractic adjustments and manual mobilization and manipulation techniques, or physical therapy may be utilized to help improve an individual’s symptoms as well as increase the strength of the surrounding structures. However, a majority of meniscal injuries may require surgical interventions to properly repair them. Researcher’s findings coincided with previous research concluded that an ACL deficient knee posed a risk to meniscus trauma but identified that this was consistent with the medial but not lateral meniscus. The authors of the research study stated that this altered consistency may be due to the medial meniscus being fixed to the joint capsule. In comparison, the lateral meniscus is not firmly attached to the joint capsule, acquiring more mobility within the joint which explains the difference in injury incidence.
It was recognized that from 3,475 individuals with previous ACL injuries, 1,638, approximately 47 percent, were diagnosed with meniscal tears. The authors added that for each month that went by for individuals that experienced an ACL rupture, there was an exponential chance of meniscal trauma of only 1 percent. Additionally, the presence of a degenerative meniscal lesion increased an individual’s risk of suffering further trauma to the knee by 1.6 to 2.0 percent.
The Risk Of Playing Sports With A Torn Meniscus
In conclusion, a wide variety of factors have been identified as potential risk components which might incline an individual to experience a greater incidence of meniscal tears. An injury to the meniscus can be sustained by anyone within the general population and athletes alike and these should not be ruled out to only develop in a single sub-group based on other research studies. Ultimately, the risk factors identified tremendously increase the chance for an individual to experience specific types of knee injuries. Although several research studies covers a large variety of risk factors for the general population and athletes, these were very limited as the majority were only supported by a few studies.
A torn meniscus can greatly affect an athlete’s optimal performance, challenging their efficiency to practice and compete in their specific sport or physical activity. As analyzed above, the gradual degeneration of the body’s structures and tissues can impact whether an athlete will suffer an injury during their lifetime. There are a variety of treatments available to help individual’s recover from a torn meniscus, such as chiropractic care, although surgical interventions have also been preferred by some athletes. Aside from the type of treatment you receive, understanding the anatomy of the meniscus and how an injury can affect it can help teach athletes on better ways to care for their sports injuries.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Sourced through Scoop.it from: www.elpasobackclinic.com
By Dr. Alex Jimenez

TRENDING TOPIC: EXTRA EXTRA: New PUSH 24/7Â®ï¸ Fitness Center
Post Disclaimer
Professional Scope of Practice *
The information herein on "The Anatomy Of An Unexpected Torn Meniscus" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness, Personal Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and our family practice-based chiromed.com site, and focuses on restoring health naturally for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Licenses and Board Certifications:
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card


 Again, We Welcome You.
Again, We Welcome You.
Comments are closed.