

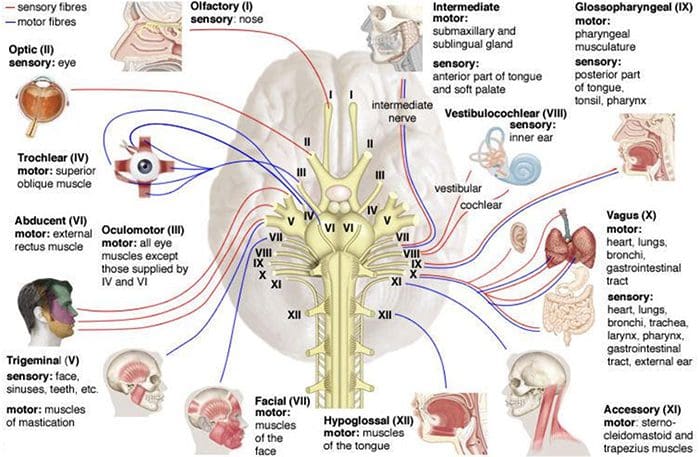
Human Cranial nerves are a set of 12 paired nerves that come directly from the brain. The first two (olfactory and optic) come from the cerebrum, with the remaining ten come from the brain stem. The names of the these nerves relate to what function they perform and are also numerically identified in roman numerals (I-XII). The nerves serve in functions of smell, sight, eye movement, and feeling in the face. These nerves also control balance, hearing, and swallowing.
Table of Contents
Cranial Nerves: Review
- CN I – Olfactory
- CN II – Optic
- CN III – Oculomotor
- CN IV – Trochlear
- CN V – Trigeminal
- CN VI – Abducens
- CN VII – Facial
- CN VIII – Vestibulocochlear
- CN IX – Glossopharyngeal
- CN X – Vagus
- CN XI – Accessory
- CN XII – Hypoglossal
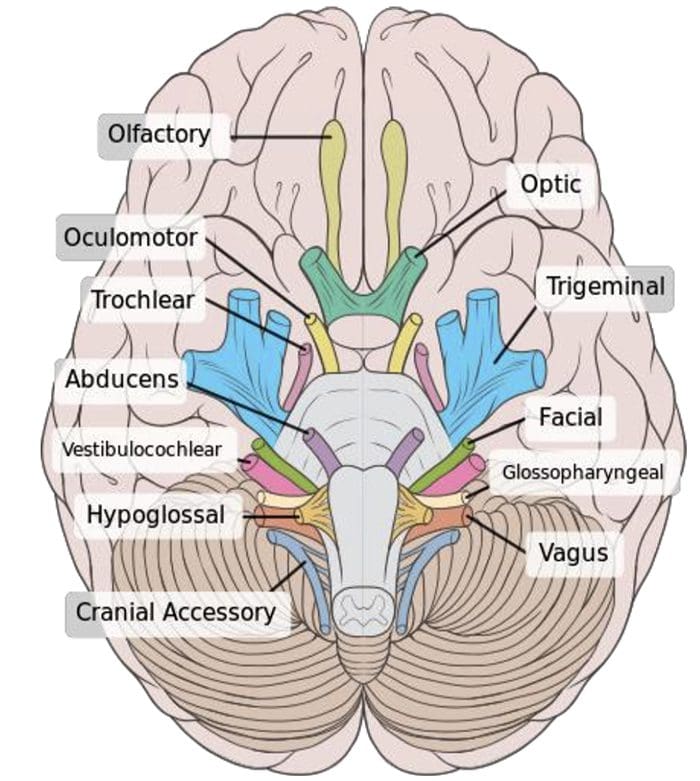
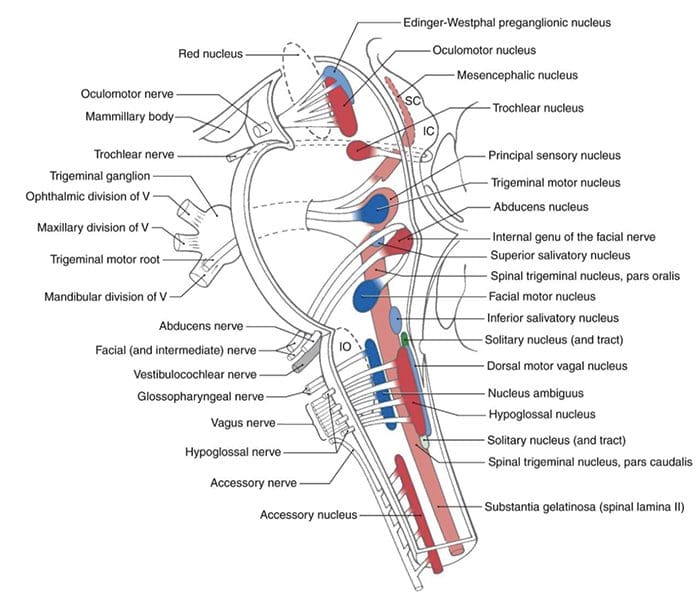
Location Of Nerves
CN I – Olfactory
 CN I Clinically
CN I Clinically
 CN I Clinically
CN I Clinically- Lesions resulting in anosmia (loss of the sense of smell) can be caused by:
- Trauma to the head, especially patient’s hitting the back of their head
- Frontal lobe masses/tumors/SOL
- Remember that loss of the sense of smell is one of the first symptoms seen in Alzheimer’s and early dementia patients
Testing CN I
- Have the patient close their eyes and cover one nostril at a time
- Have them breathe out through their nose, THEN place the scent under the nostril while they breathe in.
- Ask them “do you smell anything?â€
- This tests if the nerve is functioning
- If they say yes, ask them to identify it
- This tests if the processing pathway (temporal lobe) is functional
Cranial Nerve II – Optic
Cranial Nerve II Clinically
 Cranial Nerve II Clinically
Cranial Nerve II ClinicallyLesions to this nerve can be the result of:
- CNS disease (such as MS)
- CNS tumors and SOL
- Most problems with the visual system arise from direct trauma, metabolic or vascular diseases
- FOV lost in the periphery can mean SOL affecting the optic chiasm such as a pituitary tumor
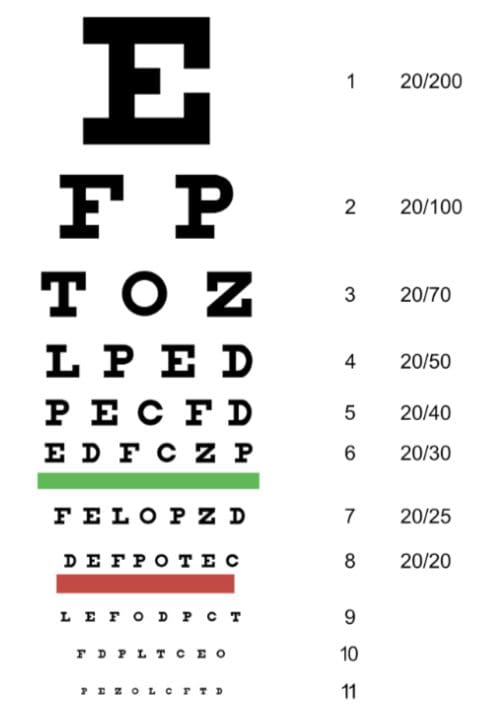
Testing Cranial Nerve CN II
-
https://upload.wikimedia.org/wikipedia/commons/9/9f/Snellen_chart.svg Can the patient see?
- If patient has vision in each eye, nerve is functional
- Visual acuity testing
- Snellen chart (one eye at a time, then two eyes together)
- Distance vision
- Rosenbaum chart (one eye at a time, then two eyes together)
- Near vision
Associated Testing For Visual System
- Ophthalmoscopic/Funduscopic exam
- Assessment of A/V ratio and vein/artery health
- Assessment of cup to disc ratio
- Field of vision testing
- Intraoccular pressure testing
- Iris shadow test
Cranial Nerve III – Oculomotor
Cranial Nerve III Clinically
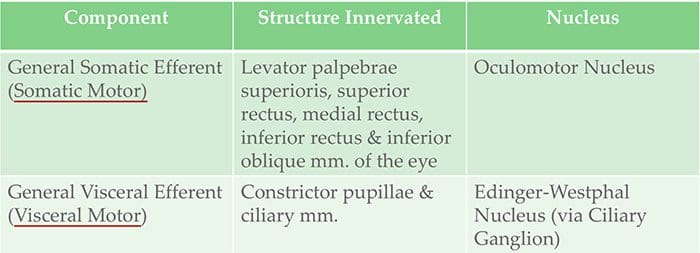 Cranial Nerve III Clinically
Cranial Nerve III Clinically- Diplopia
- Lateral strabismus (unopposed lateral rectus m.)
- Head rotation (yaw) away from the side of the lesion
- Dilated Pupil (unopposed dilator pupillae m.)
- Ptosis of the eyelid (loss of function of levator palpebrae superioris m.)
- Lesions to this nerve can be the result of:
- Inflammatory diseases
- Syphilitic and tuberculous meningitis
- Aneurysms of the posterior cerebral or superior cerebellar aa.
- SOL in the cavernous sinus or displacing the cerebral peduncle to the opposite side
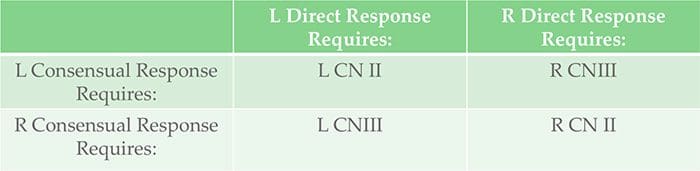
Testing Cranial Nerve CN II & III
- Pupillary reflex testing
- Move the light in front of the pupil from the lateral side and hold 6 seconds
- Watch for direct (ispilateral eye) and consensual (contralateral eye) pupillary constriction
Testing Cranial Nerve CN II & III
 Testing Cranial Nerve CN II & III
Testing Cranial Nerve CN II & III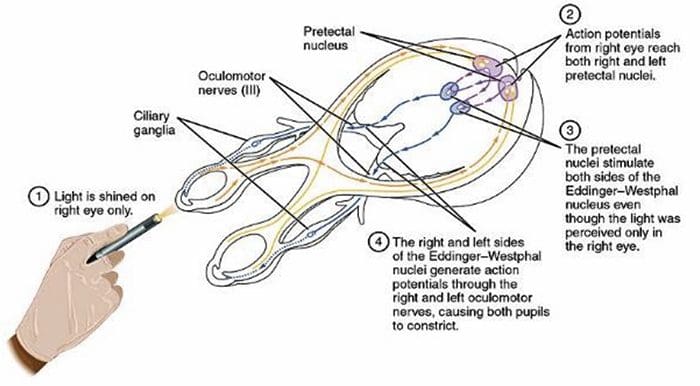
Cranial Nerve IV – Trochlear
Cranial Nerve IV Clinically
 Cranial Nerve IV Clinically
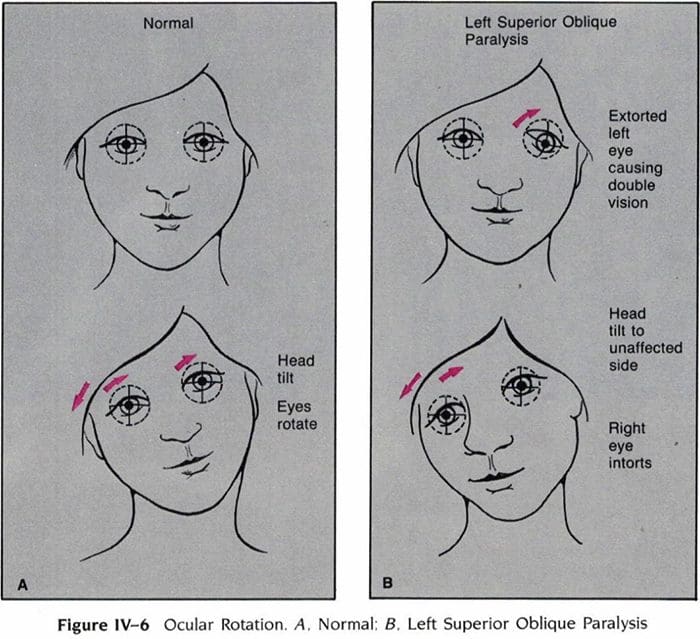
Cranial Nerve IV Clinically- Patient has diplopia & difficulty in downward gaze
- Often complain of difficulty walking down stairs, tripping,falling
- Extortion of the affected eye (unopposed inferior oblique m.)
- Head tilt (roll) to the unaffected side
- Lesions to this nerve can be the result of:
- Inflammatory diseases
- Aneurysms of the posterior cerebral or superior cerebellar aa.
- SOL in the cavernous sinus or superior orbital fissure
- Surgical damage during mesencephalon procedures
Head Tilt In Superior Oblique Palsy (CN IV Failure)
Cranial Nerve VI – Abducens
Cranial Nerve VI Clinically
 Cranial Nerve VI Clinically
Cranial Nerve VI Clinically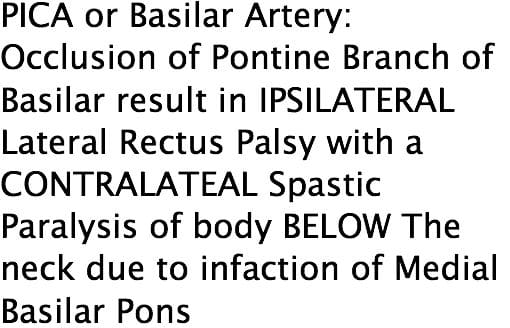
- Diplopia
- Medial strabismus (unopposed medial rectus m.)
- Head rotation (yaw) toward the side of the lesion
- Lesions to this nerve can be the result of:
- Aneurysms of the posterior inferior cerebellar or basilar aa.
- SOL in the cavernous sinus or 4th ventricle (such as a cerebellar tumor)
- Fractures of the posterior cranial fossa
- Increased intracranial pressure
Testing Cranial Nerve CN III, IV & VI
- H-Pattern testing
- Have the patient follow an object no larger than 2 inches
- Patient’s can have focus difficulty if the item is too large
- It’s also important not to hold the object too close to the patient.
- Convergence and accommodation
- Bring object close to the bridge of the patient’s nose and back out. Perform at least 2 times.
- Look for pupillary constriction response as well as convergence of the eyes
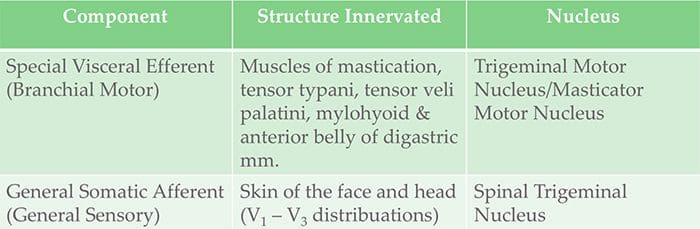
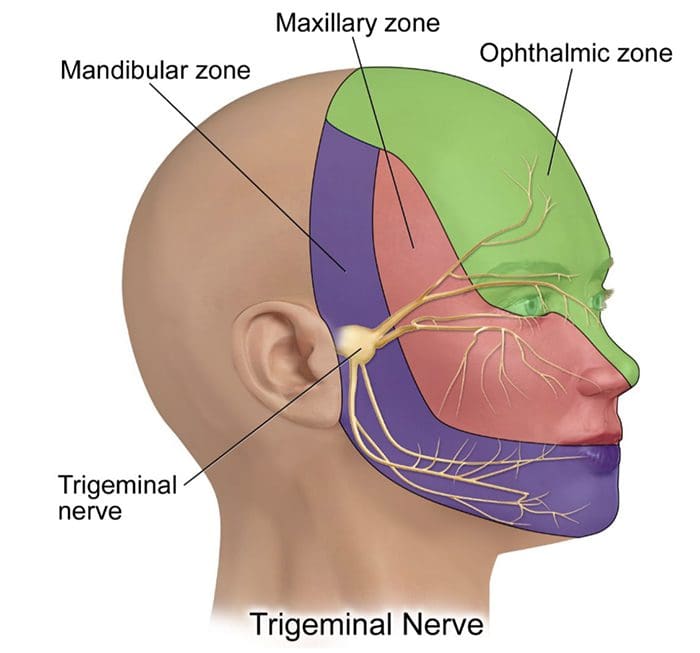
Cranial Nerve V – Trigeminal
Cranial Nerve V Clinically
 Cranial Nerve V Clinically
Cranial Nerve V Clinically- Decreased bite strength on the ipsilateral side of lesion
- Loss of sensation in V1, V2 and/or V3 distribution
- Loss of corneal reflex
- Lesions to this nerve can be the result of:
- Aneurysms or SOL affecting the pons
- Specifically tumors at the cerebellopontine angle
- Skull fractures
- Facial bones
- Damage to foramen ovale
- Tic doloureux (Trigeminal neuralgia)
- Sharp pain in V1-V3 distributions
- Tx with analgesic, anti-inflammatory, contralateral stimulation
Testing Cranial Nerve CN V
- V1 – V3 pain & light touch testing
- Testing is best done toward the more medial or proximal areas of the face, where V1, V2 &V3 are better delineated
- Blink/Corneal reflex testing
- Puff of air or small tissue tap from the lateral side of the eye on the cornea, if normal, the patient blinks
- CN V provides the sensory (afferent) arc of this reflex
- Bite strength
- Have patient bite down on tongue depressor & try to remove
- Jaw jerk/Masseter Reflex
- With patient’s mouth slightly open place thumb on patient’s chin and tap your own thumb with a reflex hammer
- Strong closure of the mouth indicates UMN lesion
- CN V provides both the motor and sensory of this reflex
Cranial Nerve VII – Facial
Cranial Nerve VII Clinically
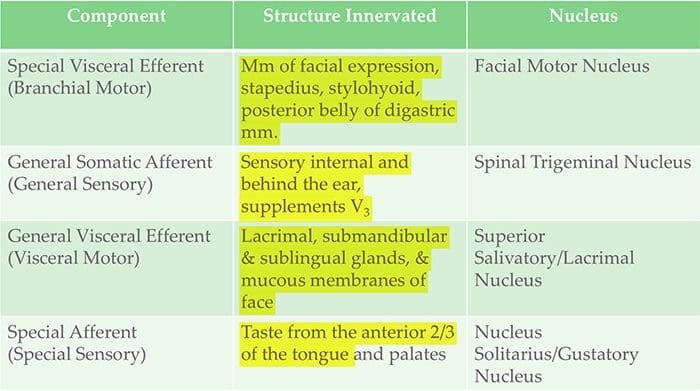 Cranial Nerve VII Clinically
Cranial Nerve VII Clinically- As with all nerves, symptoms describe the location of the lesion
- Lesion in the lingual nerve will result in loss of taste, general sensation in tongue & salivary secretion
- Lesion proximal to the branching of the chorda tympani such as in the facial canal will result in the same symptoms without the loss of general sensation of the tongue (because V3 has not yet joined the CN VII)
- Corticobulbar innervation is asymmetric to the upper and lower parts of the Facial Motor Nucleus
- If there is an UMN lesion (lesion to the corticobulbar fibers) the patient will have paralysis of the muscles of facial expression in the contralateral lower quadrant
- If there is a LMN lesion (lesion to the facial nerve itself) the patient will have paralysis of the muscles of facial expression in the ipsilateral half of the face
- Bell’s Palsy
Testing Cranial Nerve CN VII
- Ask the patient to mimic you or follow instructions to make certain facial expressions
- Be sure to assess all four quadrants of the face
- Raise eyebrows
- Puff cheeks
- Smile
- Close eyes tightly
- Check for strength of the buccinator muscle against resistance
- Ask patient to hold air in their cheeks as you press gently from the outside
- Patient should be able to hold air in against resistance
Cranial Nerve VIII – Vestibulocochlear
Cranial Nerve VIII Clinically
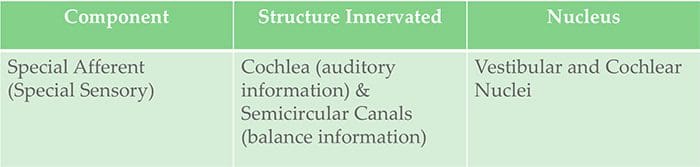 Cranial Nerve VIII Clinically
Cranial Nerve VIII Clinically- Changes in hearing alone are most often due to
- Infections (otitis media)
- Skull fracture
- The most common lesion to this nerve is caused by an acoustic neuroma
- This affects CN VII and CNVIII (cochlear AND vestibular divisions) due to proximity in the internal auditory meatus
- Symptoms include nausea, vomiting, dizziness, hearing loss, tinnitus, and bell’s palsy etc.
Testing Cranial Nerve CN VIII
- Otoscopic Exam
- Scratch Test
- Can the patient hear equally on both sides?
- Weber Test
- Tests for lateralization
- 256 Hz tuning fork placed on top of the patient’s head in the center, is it louder on one side than the other?
- Rinne Test
- Compares air conduction to bone conduction
- Normally, air conduction should last 1.5-2 as long as bone conduction
Testing Cranial Nerve CN VIII

Cranial Nerve IX – Glossopharyngeal
Cranial Nerve IX Clinically
 Cranial Nerve IX Clinically
Cranial Nerve IX Clinically- This nerve is rarely damaged alone, due to it’s proximity to CN X & XI
- Look for signs of CN X & XI damage as well if CN IX involvement is suspected
Cranial Nerve X – Vagus
Cranial Nerve X Clinically
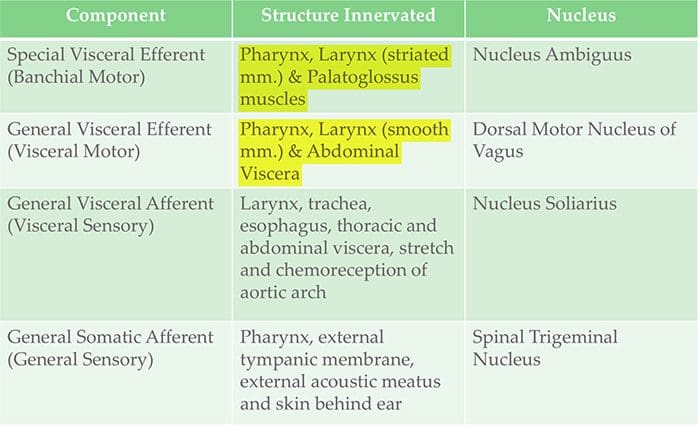 Cranial Nerve X Clinically
Cranial Nerve X Clinically- Patient may have dysarthria (difficulty speaking clearly) and dysphagia (difficulty swallowing)
- May present as food/liquid coming out their nose or frequent choking or coughing
- Hyperactivity of the visceral motor component can cause hypersecretion of gastric acid leading to ulcers
- Hyper-stimulation of the general sensory component can cause coughing, fainting, vomiting and reflex visceral motor activity
- The visceral sensory component of this nerve only provides general feelings of un-wellness, but visceral pain is carried on the sympathetic nerves
Testing Cranial Nerve IX & X
- Gag reflex
- CN IX provides the afferent (sensory) arc
- CN X provides the efferent (motor) arc
- ~20% of patients have a minimal or absent gag reflex
- Swallowing, gargling, etc.
- Requires CN X function
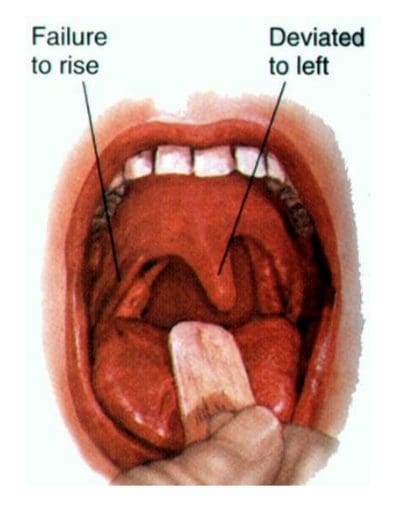
- Palatal elevation
- Requires CN X function
- Is it symmetrical?
- Palate elevates and uvula deviates contralateral to damaged side
- Auscultation of the heart
- R CN X innervates SA node (more rate regulation) and L CN X the AV node (more rhythm regulation)
Cranial Nerve XI – Accessory
Cranial Nerve XI Clinically
 Cranial Nerve XI Clinically
Cranial Nerve XI Clinically- Lesions may result from radical surgeries in the neck region, such as removal of laryngeal carcinomas
Testing Cranial Nerve XI
- Strength test SCM m.
- Patient will have difficulty turning head against resistance toward the side opposite of the lesion
- Strength test trapezius m.
- Patient will have difficulty with shoulder elevation on the side of the lesion
Cranial Nerve XII – Hypoglossal
Cranial Nerve XII Clinically
 Cranial Nerve XII Clinically
Cranial Nerve XII Clinically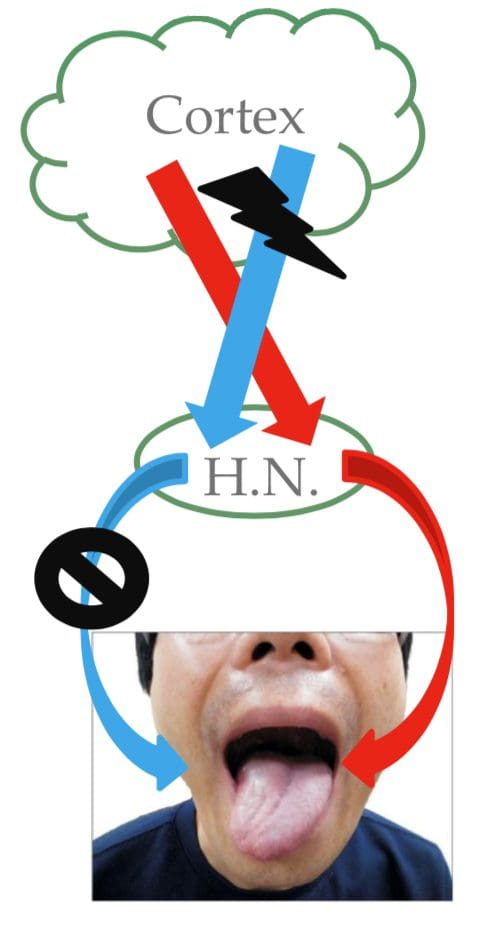
- On tongue protrusion, the tongue deviates toward the side of the inactive genioglossus m.
- This could be contralateral to a corticobulbar (UMN) lesion OR ipsilateral to a hypoglossal n. (LMN) lesion
Testing Cranial Nerve XII
- Ask patient to stick out their tongue Look for deviation as in above slide
- Have patient place tongue inside cheek and apply light resistance, one side at a time
- Patient should be able to resist moving the tongue with pressure
Clinical Examination – CN’s I – VI (Lower CN’s)
Clinical Examination – CN’s VII – XII
Sources
Blumenfeld, Hal. Neuroanatomy through Clinical Cases. Sinauer, 2002.
Pauwels, Linda Wilson, et al. Cranial Nerves: Anatomy and Clinical Comments. Decker, 1988.
Post Disclaimer
Professional Scope of Practice *
The information herein on "Cranial Nerves: Introduction | El Paso, TX." is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness, Personal Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and our family practice-based chiromed.com site, and focuses on restoring health naturally for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Licenses and Board Certifications:
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card


 Again, We Welcome You.
Again, We Welcome You.
Comments are closed.