


Table of Contents
Hip Fractures
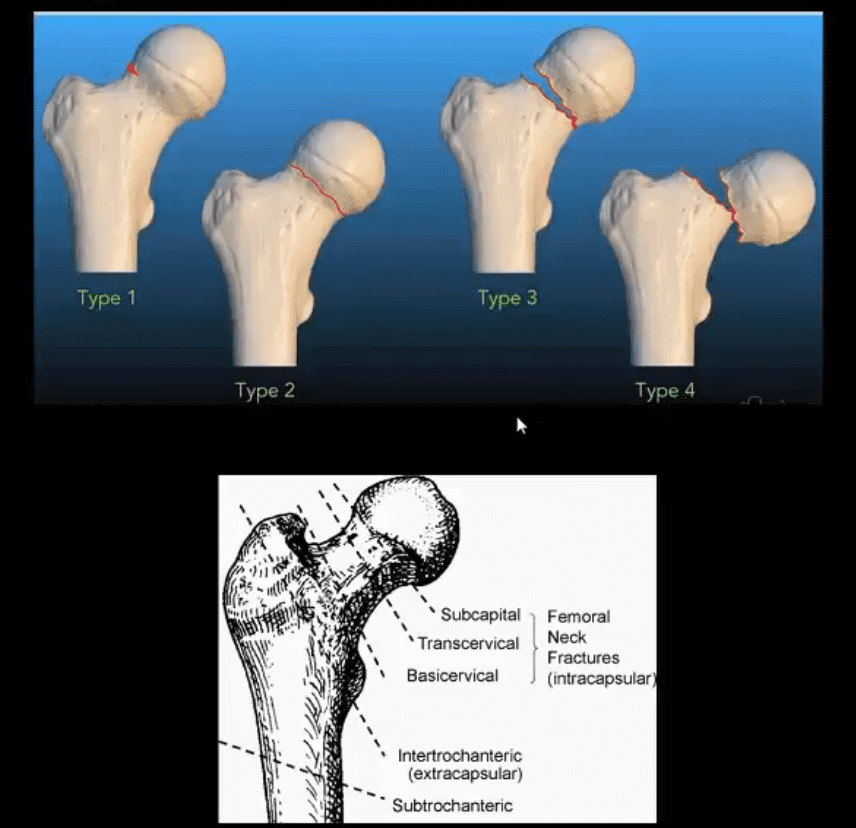
- Garden Classification (above) helps with Dx and correct management of patients
- M/C Fx are subcapital (80%)
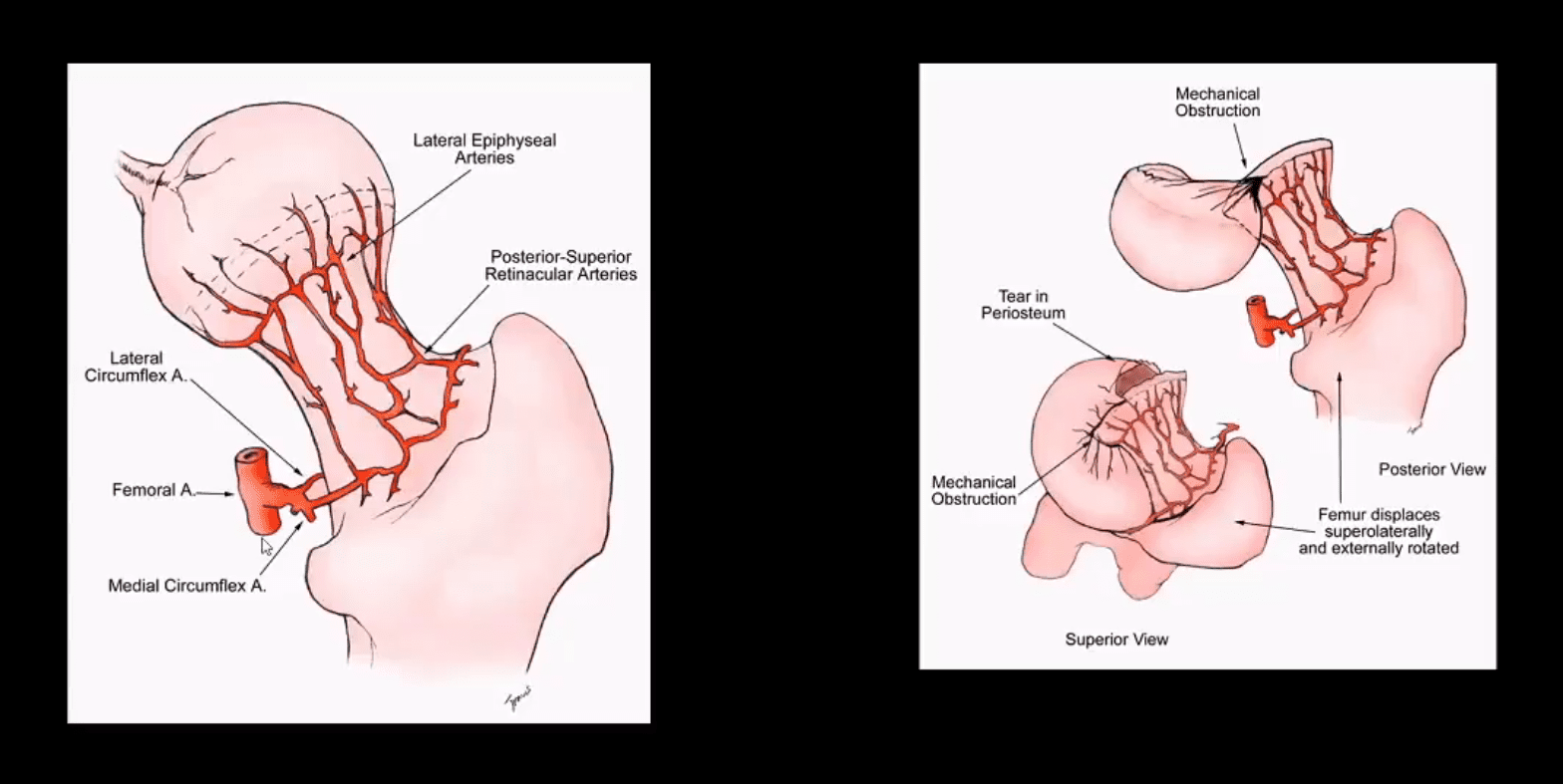
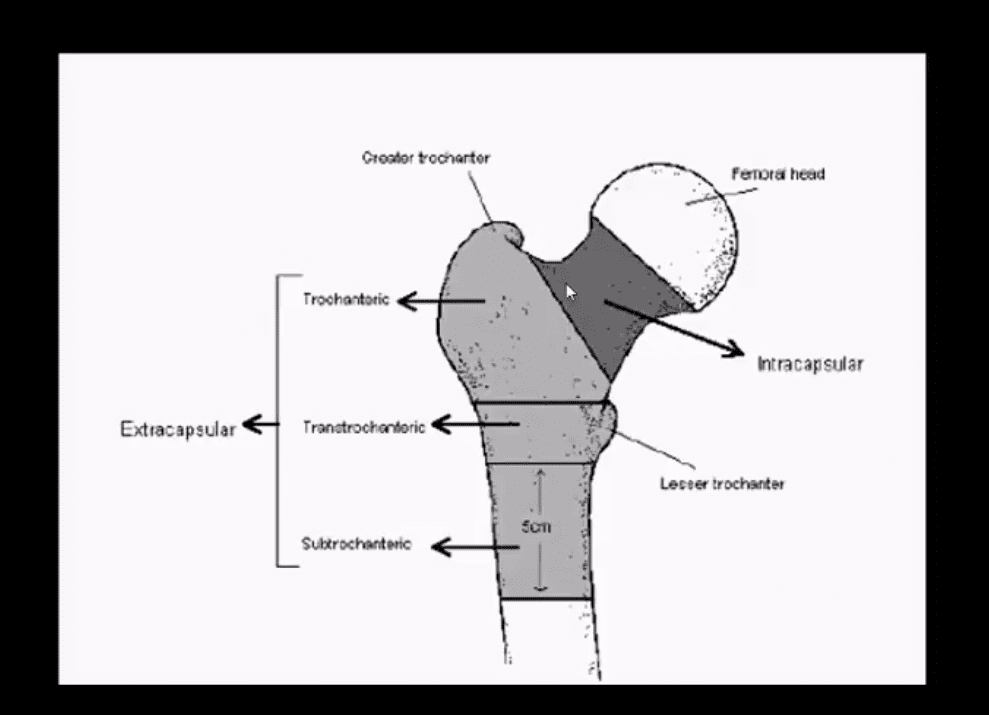
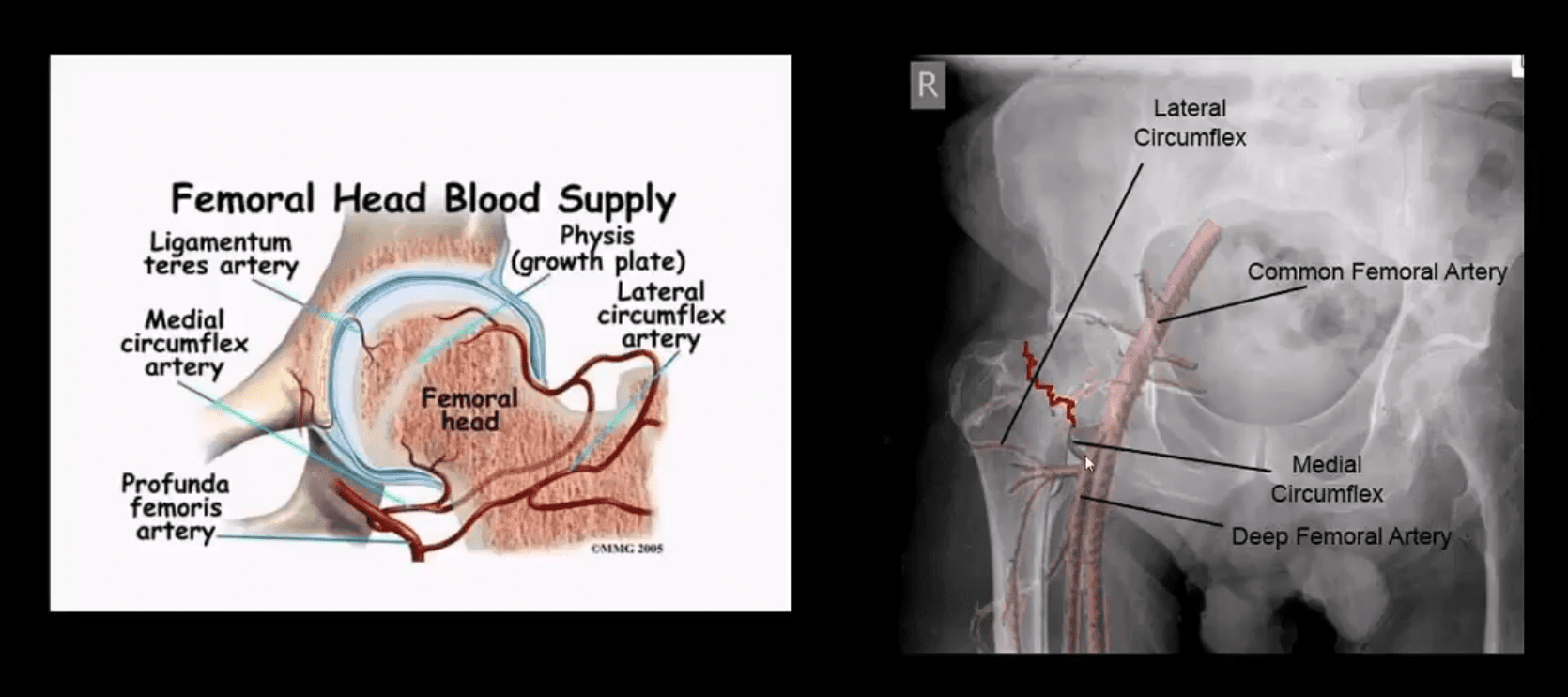
- Fxs differentiated as intra-capsular (high risk of AVN) & extra-capsular (lower risk of AVN)
- Garden 1: incomplete undisplaced Fx typically impaction with valgus off-set of the head (15-20% AVN) patient able to ambulate
- Garden 2: complete, undisplaced Fx (30% AVN)
- Garden 3: complete, partially <50% displaced
- Garden 4: complete, 100% displaced Fx, pt collapsed with entire LE in ER (below image)
- Most osteoporotic Fx are intracapsular
Complete Displaced Femoral Neck Fracture Clinical Presentation

Imaging: Begins with X-radiography with Most Fxs
- CT scanning may help with further delineation of Fx complexity/displacement and Dx of additional regional Fxs
- MRI can be helpful if x-radiography fails to Dx fx
- X-radiography pitfalls: some undisplaced Garden 1 & 2 Fxs may be missed d/t pre-existing DJD and osteophytes along the femoral head-neck junction that may overly the Fx line
- Fx line is incomplete and too small/subtle especially if the study is read by non-radiologists
- Incomplete Fxs if left untreated will not heal and likely to progress to complete Fxs
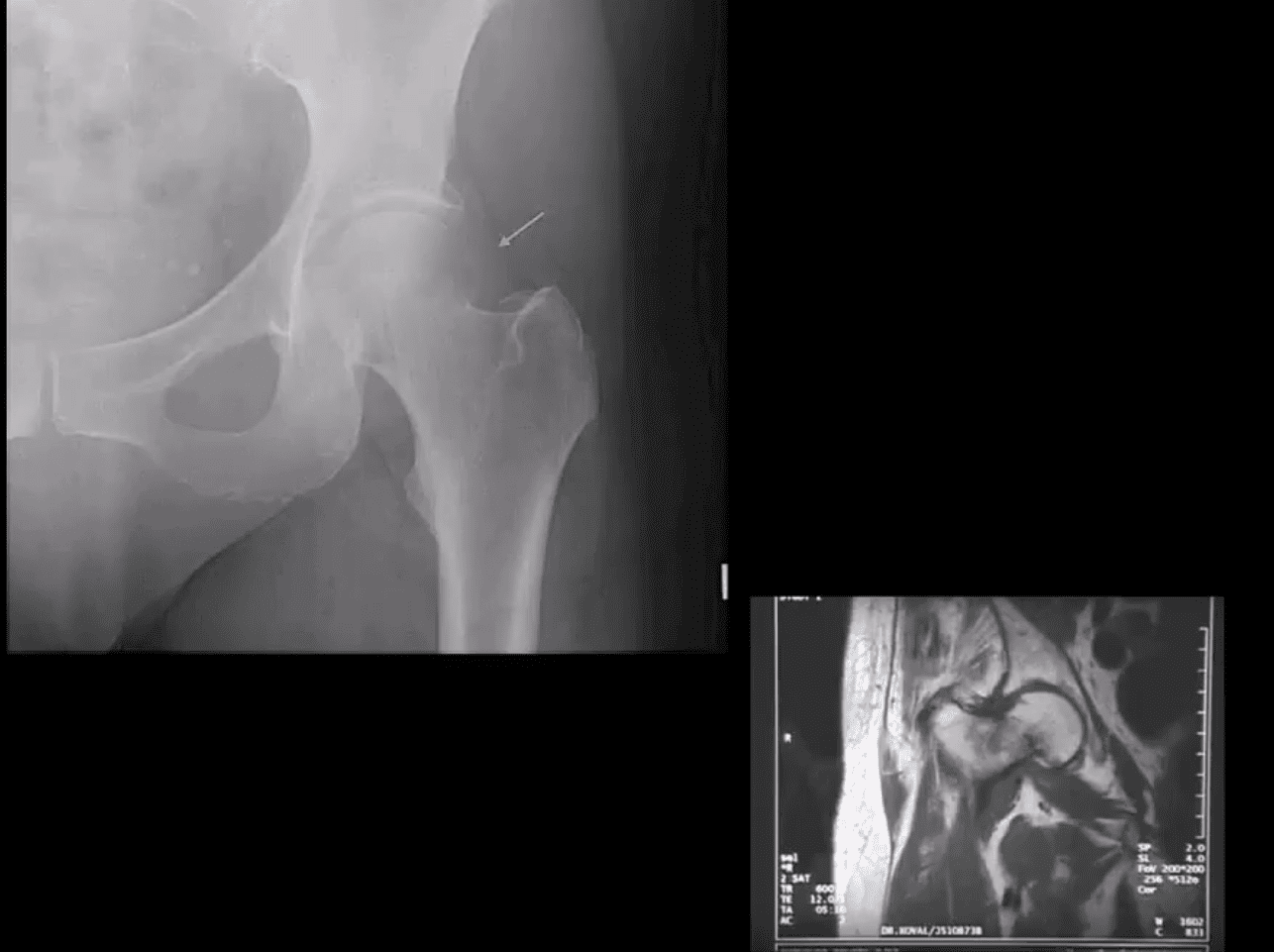
- AP hip spot view: note valgus deformity of the head (above yellow arrow) with a small/subtle line of sclerosis in the sub-capital region representing Garden 1 Fx. MRI may help with Dx of subtle radiographic Fxs. If MRI contraindicated, Tc 99 radionuclide bone scan may help demonstrate high uptake of the radiopharmaceutical in Fx (below image)
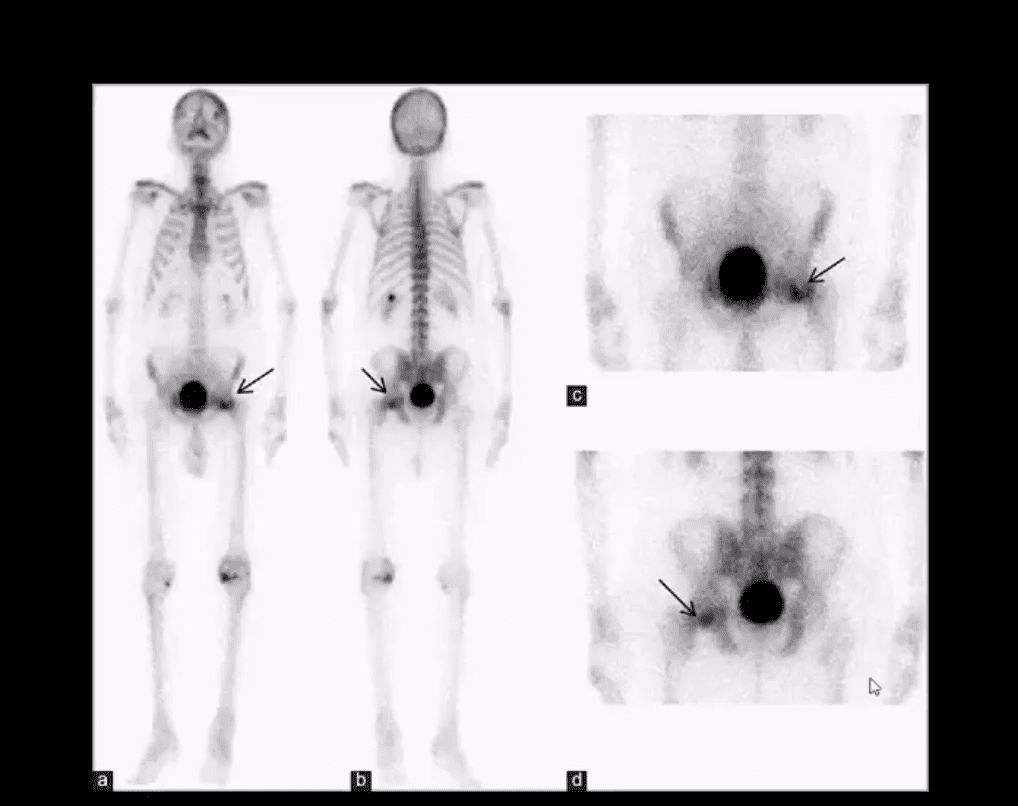
Above – Tc99 Radionuclide Bone Scan Reveals Left Subcapital Femoral Neck Fx
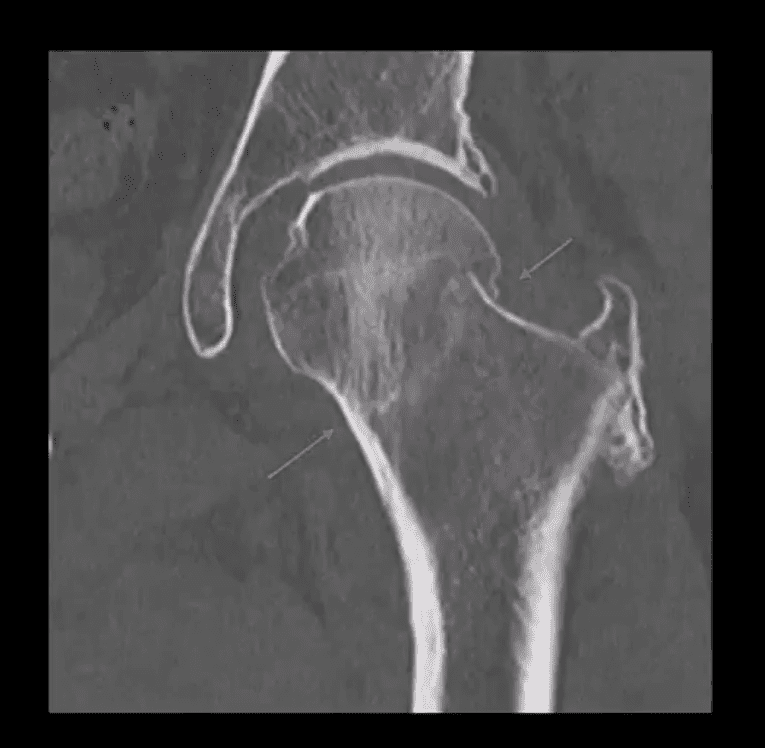
- Garden 2 complete undisplaced (above green arrows) Fx
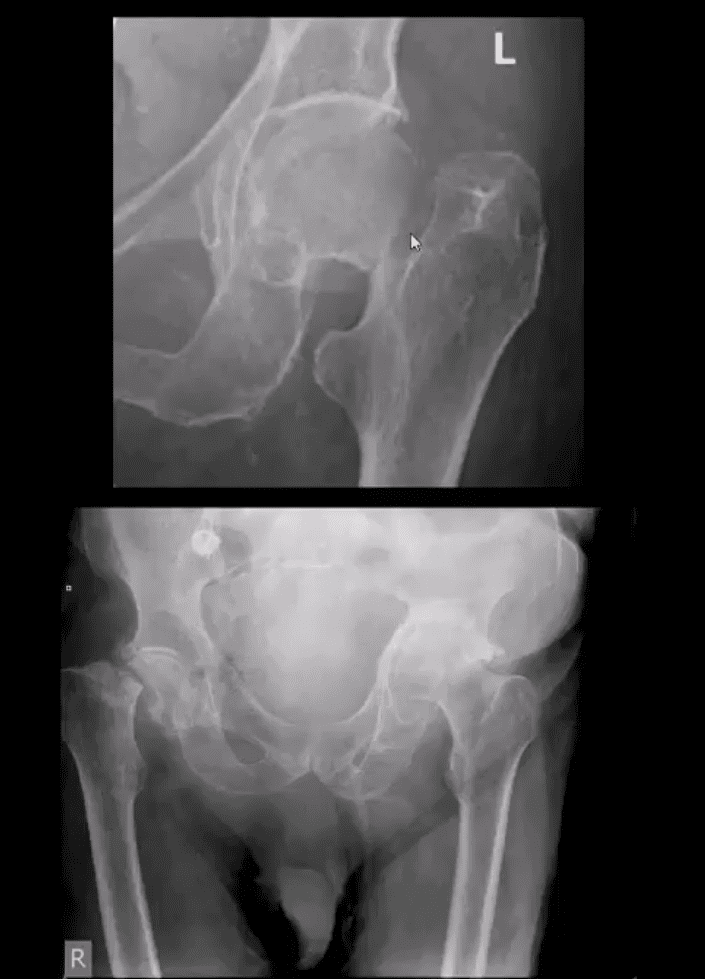
- AP hip: Garden 3 complete partially displaced Fx (above the first image)
- AP pelvis: complete displaced Garden 4 Fx (above the second image)
- Clinical pearls: in some cases of Garden 4 Fx, DDx may be difficult to differentiate from OSP vs. pathologic fx d/t to bone Mets of Multiple myeloma (MM)
- Management: depends on patients age and activity level
- Garden 3 & 4 require total hip arthroplasty in patients <85-y.o.
- Garden 1 & 2 may be treated with closed reduction of fx and open capsule and 3-cannulated fixating screws
- Pre-existing DJD may require total arthroplasty
- Occasionally observation may be performed on patients who are not active and significant risks of surgery and depends on surgical centers
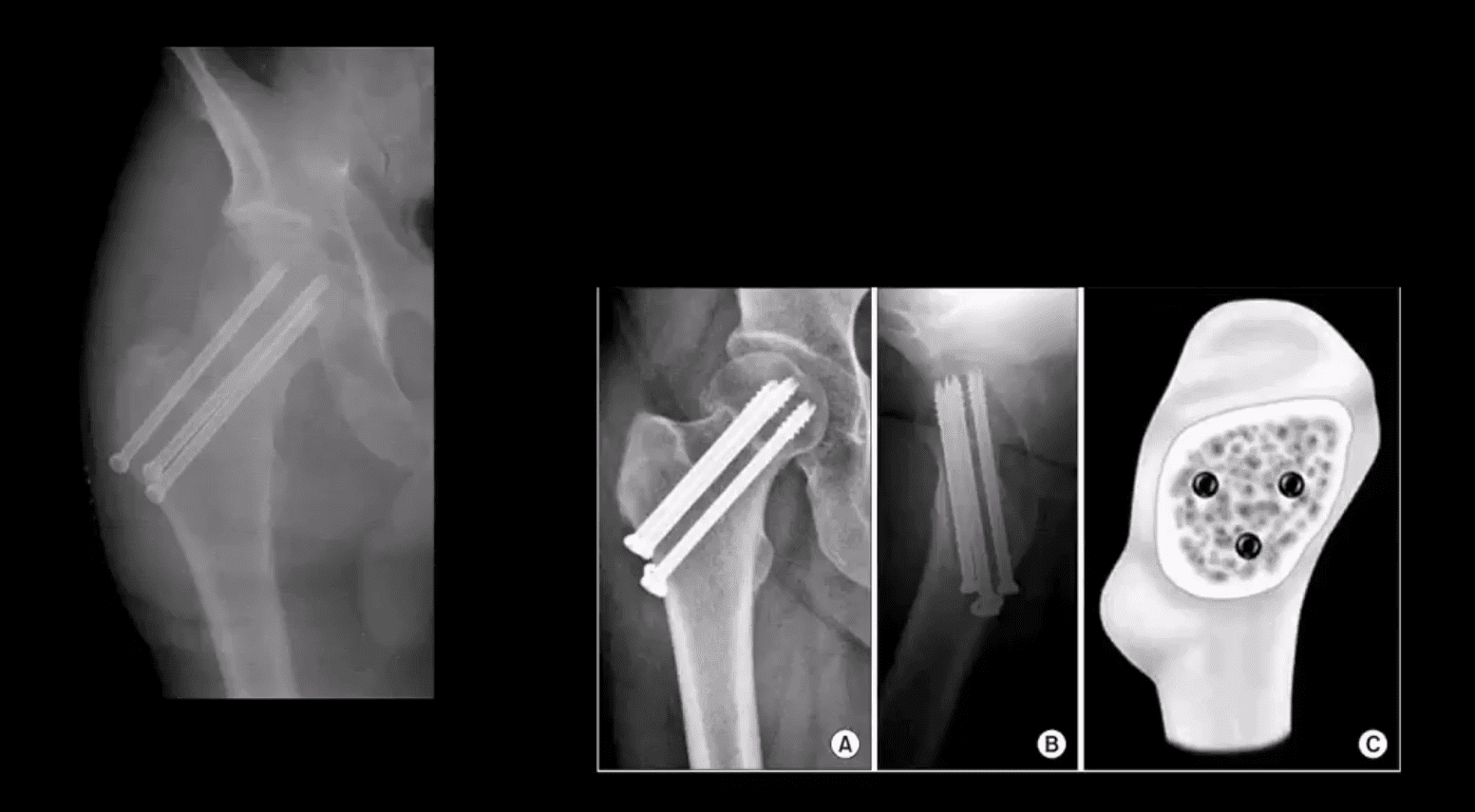
- m/c Rx of Garden 1 & 2 undisplaced Fx with 3-screws. Screws proximity depends on the bone quality and Fx type
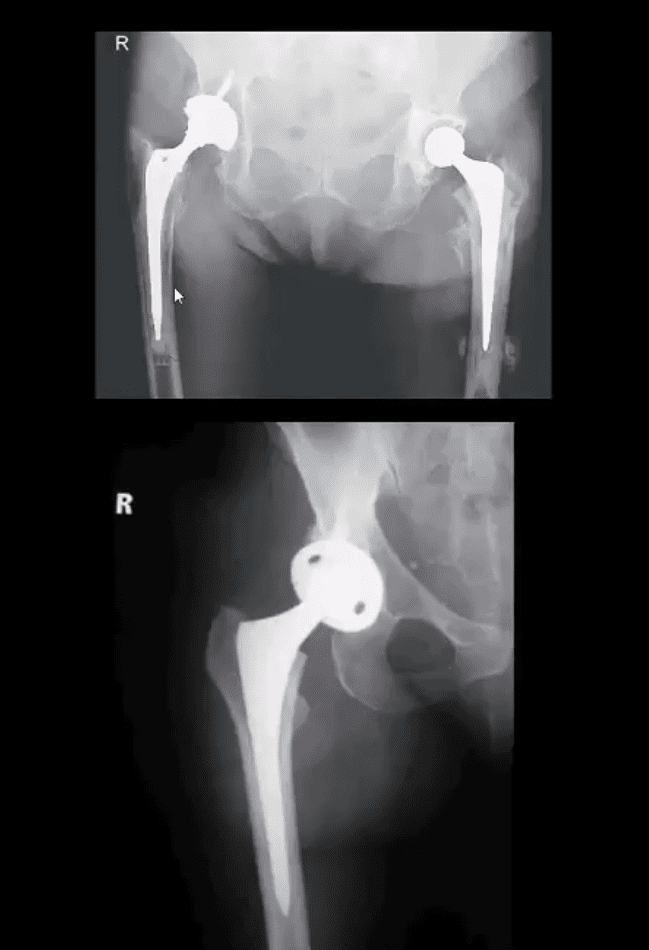
- THA aka hip replacement: cemented THA with bone cement (above the first image) vs. non-cemented (biologic) that is used mostly in younger patients
- 2-types: metal on metal vs. metal on polyethylene
- The femoral angle of the prosthesis should have slight valgus but never >140 degrees
- The non-cemented component uses porous metal allowing the bone to integrate sometimes coating in bone cement from osteoconduction
- THA has good outcome and prognosis
- Occasionally cement failure, fractures, and infections may complicate this procedure
Supplemental Reading
- https://www.aafp.org/afp/2014/0615/p945.html
- https://emedicine.medscape.com/article/87043-overview
- https://radiopaedia.org/articles/proximal-femoral-fractures-summary
Acute Pelvis & Hip Trauma
Post Disclaimer
Professional Scope of Practice *
The information herein on "Acute Pelvis & Hip Trauma Imaging Diagnosis Part II | El Paso, TX." is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness, Personal Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and our family practice-based chiromed.com site, and focuses on restoring health naturally for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933


 Again, We Welcome You.
Again, We Welcome You.
Comments are closed.